Symptom Remission and Improved WBC and RBC Counts in 30 Men with Chronic Genitourinary Complaints Treated with Repetitive Prostatic Massage, Antimicrobials, and Medical Therapy
Bradley R. Hennenfent , Noel E. de Vera, and Antonio Espinosa Feliciano, Jr.
Abstract
Background
The Manila Genitourinary Clinic treats men with chronic urogenital complaints with repetitive prostatic massage, antimicrobial therapy, and sometimes with urologic medications.
Methods
We performed a retrospective chart review of 30 men (mean age, 51.33; range,
26–76; SD, 14.19), presenting for the first time with genitourinary complaints of more than 3 months duration. Urethral smears, expressed prostatic secretions (EPS), and post-massage urinalyses were collected 514 times (mean number of specimens, 17.13; range, 10–35; SD, 4.80). Importantly, EPS was obtained in
100% of attempts.
Results
Ninety percent (27 of 30) of the men improved during treatment; the mean global symptom severity score dropped from 6.40 (range, 3–10; SD, 2.04) at the first visit to 1.95 (range, 0–9; SD, 2.24) at the last visit, a 69.53% reduction, which was statistically significant (mean difference, 4.44; 95% confidence interval [CI],
3.37 – 5.52); t(29) = 8.47; P < 0.0001). Ten patients (33.33%) reported complete remission of their symptoms by their last visit, which was also significant (P <
.0005). Statistically significant declines occurred in first to last urethral WBC counts, peak to last EPS WBC and RBC counts, and peak to last post-massage urinary WBC and RBC counts. In only 3 of 30 men (10%) was the first EPS specimen the most purulent specimen obtained. The highest number of EPS WBC peaks occurred at the sixth prostatic massage. Twenty-nine of the 30 men (96.67%) had an EPS WBC count of 5 per oil immersion field (1000X magnification) by the eighth prostatic massage. Ten prostatic massages were necessary to obtain over 80 percent of the EPS WBC peaks. Urethral WBC peaks occurred earlier in therapy than EPS and post-massage urinary WBC peaks. Patients who responded best to therapy more often had Chlamydia
elementary bodies seen and tended to be more purulent in urethral smears, EPS, and post-massage urines. Conclusions
In these 30 men with chronic urogenital complaints, repetitive prostatic massage combined with antimicrobial therapy resulted in significantly improved symptom scores, complete remission of symptoms in 33% of men, and statistically significant improvements in WBC and RBC counts. We recommend a minimum of 10 prostatic massages in order to obtain the most purulent specimens for analysis and disease classification, as well as for therapeutic reasons. We describe a non-invasive method of obtaining urethral smears. We also recommend microbial testing, including Chlamydia testing, and we recommend testing BPH patients for prostatitis.
Key words: prostatitis, benign prostatic hyperplasia (BPH), urethritis, chronic pelvic pain syndrome, CPPS, transurethral resection of the prostate, TURP, transurethal resection, TUR, Chlamydia, Chlamydia trachomatis, C. trachomatis.
Introduction
Since the 1970s, physicians in Manila, Philippines have been treating chronic urogenital complaints with repetitive prostatic massage.
Dr. Antonio Espinosa Feliciano, Jr., M.D., has previously reported seeing a rise and fall of EPS WBC counts in patients with chronic prostatitis during therapy with repetitive prostatic massage, theoretically due to the release of obstructed, pus-filled, prostatic acini. He calls this phenomenon “the clinical horizon.” The
clinical horizon was documented in our previous paper.[1] We are also interested in other WBC and RBC changes during treatment and wondered which specimens collected from urethral smears, the EPS, and the post-massage urine would provide the most purulent samples for analysis.
Patients and Methods
Forty-three patients’ charts were selected randomly from 1999 to 2001 for retrospective review. Patients were included in the study if it was their first time to the clinic and if they had chronic urogenital symptoms consistent with prostatitis
of more than three months duration. None of these patients’ charts had been reviewed for any previous study.
Thirteen patients were excluded from the chart review. Six patients were excluded because they did not complete at least 10 prostatic massages. Three patients were excluded because they had been previously treated at the clinic; all study patients are first-time patients. Two patients were excluded because they presented with a chief complaint of infertility and were without pelvic pain or urinary symptoms. One patient was excluded because his chief complaint was pustular lesions of the genitalia. Another patient was excluded because his chief complaint was vesicular lesions of the coronal sulcus. In the 13 excluded
patients, the global symptom score dropped from 3.92 to 2.08 by the end of treatment, a 47% improvement.
Patients with a complaint of urethral discharge or those who had urethral discharge visible on physical exam were to be excluded but there were no such cases. After the exclusions, 30 men were left for retrospective chart review. Thirty was targeted as a number that would reach significance based on our earlier study.
Symptoms were tabulated into 1 of 4 categories: pelvic pain, irritative urinary symptoms, obstructive urinary symptoms, or sexual dysfunction. Patients were asked to self-assess their global symptom severity score at each clinic visit on a scale of 0 to 10, with zero being no symptoms and 10 being the worst possible symptoms. If a patient gave a range for his symptom score, the average was used. A few patients used exact decimal places when reporting their symptom scores. The National Institutes of Health Chronic Prostatitis Symptom Index was not available in the Tagalog language for use in this study.
The rapid plasma reagent test for syphilis (Randox) and the Treponema palladium heme agglutination tests (HUMAN) were done on all 30 patients’ blood specimens, and these two syphilis tests were negative in all cases.
After milking the penis at least 5 times, urethral smears were done on all patients by pressing a glass slide against the patient’s urethral mucosa. This technique, which is painless for the patient, is used instead of inserting swabs inside the urethra. No cleaning was done prior to obtaining the urethral smears, which were Gram-stained. Urethral bacteria were recorded as Gram-positive cocci (GPC), Gram-positive bacilli (GPB), Gram-negative cocci (GNC), and Gram-negative bacilli (GNB). The urethral smear WBC count was counted under oil immersion at
1000 times magnification and reported as a range from low to high. We used the high counts in our analysis.
Repetitive prostatic massage was performed on all patients on at least a thrice- weekly schedule. If cultures were going to be taken, the periurethral area was cleaned with isopropyl alcohol prior to the massage.
After massage, the drop of EPS hanging at the end of the penis was Gram- stained by laboratory technicians. Ranges of WBC counts and RBC counts from low to high were recorded. The high counts were used in our analysis. The counting of EPS WBCs and RBCs was done under microscopy at 1000X magnification. Microscopic fields, which contained clumps of WBCs, were not used during the counting process. When the number of EPS WBCs were too numerous too count, the number was recorded as 60, an artificial limit. Thus, the Clinic’s WBC counting technique is conservative and results in the undercounting of EPS WBCs in some cases.
After the first drop was taken for Gram-staining, an additional drop of EPS was taken for staining with Tb-fluor (Merck), which was examined under oil immersion
at 1000 power magnification. All 30 men were negative for tuberculosis according to the Tb-fluor test results.
The penis was milked of the remaining prostatic fluid, which was sent for culture after the first massage and sometimes after later massages at the discretion of the treating physician and the patient. One complete set of cultures of the EPS was performed prior to the administration of antibiotics in all 30 patients. Aerobic
organisms were cultured with brain heart infusion broth. Anaerobes were cultured with cooked-meat medium. Trichomonas broth was used to culture for Trichomonas and other flagellates. Mycoplasma IST2 broth was used to culture for Ureaplasma and Mycoplasma.
Immediately after the first EPS collection, a cotton swab was inserted into the urethra to collect mucosal cells for Chlamydia trachomatis testing, which was performed by direct fluorescent antibody (DFA) technique. The DFA tests were by BioMérieux or Trinity Biotech, depending on supply and availability. C. trachomatis DFA testing was sometimes repeated during treatment at the discretion of the treating physician and the patient. Elementary bodies were quantified and determined by color, shape, intensity, and size. We considered the test results positive if any C. trachomatis fluorescing elementary bodies were seen and recorded the number. A previous study[2] and our ongoing clinical experience suggest that even one fluorescing elementary body found by DFA may be significant. The manufacturers, however, recommend that 10 or more fluorescing elementary bodies be considered a positive test result. When C. trachomatis fluorescing elementary bodies were seen, each man was counseled
to have his sexual partner or partners examined, tested, and if indicated, treated. All 30 patients were asked to refrain from unprotected sexual activity during the treatment period. Only 1 patient, patient No. 8, did not have at least 1 Chlamydia DFA test performed.
After prostatic massage, each patient was asked to urinate 10 milliliters of his first flow into a sterile container for urinalysis. This sample corresponds to the voided bladder 3 (VB3) specimen from the historic Meares and Stamey 4 glass localization protocol and is generally thought to reflect the EPS.[3] A standard urinalysis was then performed. However, when the number of urinary WBCs was too numerous too count, the number recorded was 60, an artificial ceiling. Thus, our WBC counting technique resulted in the undercounting of post-massage urinary WBCs in some cases.
All the laboratory tests and microscopy work were done by certified laboratory technicians independently of the treating physicians.
Statistics
Descriptive statistics were used to organize the data through the computation of means, frequencies, and percentage distributions. We used the mean for
descriptive purposes for consistency, while including all the raw data. There were no data missing from the urethral WBC counts, urethral RBCs, EPS WBCs, EPS RBCs, urine WBCs, or the urine RBCs. Of 514 opportunities at clinic visits to record symptom scores, only 12 scores were missing from the charts. These
were all from 2 patients and were missing from the middle of therapy, except for one data point missing at the end of one patient’s treatment, therefore, the second to last symptom score was used in the analysis in that instance.
Kurtosis and skewness analyses demonstrated the symptom scores at presentation to be normally distributed. Therefore, we compared the means of the first and last symptom scores using paired t-tests.
However, kurtosis and skewness analyses suggested that the patients’ cell counts were not normally distributed. In addition, the possibility of normal distribution was prevented in the EPS and urinary WBC data by the artificial ceiling of 60 cells per microscopic field under 1000X magnification.
The Friedman test was used to compare 3 related samples with P values less than 0.05 being considered significant. Friedman testing was followed by the non-parametric Wilcoxon signed ranks test (two-tailed) to compare 2 related samples, using a simplified Bonferroni correction with less than 0.017 being
considered significant. For the WBC counts, these calculations would tell us if the clinical horizon existed and whether or not the first specimen was the most purulent specimen collected during treatment.
If the Friedman test showed that there was a difference between 3 samples, but the data did not achieve significance on post-hoc Wilcoxon tests, we assumed that the Wilcoxon test pair with the smallest P value indicated the 2 samples that caused the Friedman’s test to be significant in the first place.
We recognize that comparing signed ranks has less statistical power than comparing means; however, our data was not normally distributed and comparing signed ranks would tend to compensate for the artificial ceiling of 60 cells in the EPS and urinary WBC counts.
To compare two independent groups with differing numbers of N based on ranked scores we used the Mann-Whitney test.
When looking at data peaks, if more than 1 peak occurred, the first peak was used for numerical analysis, while, to prevent bias, all peaks were used when graphing temporal relationships of peaks.
All statistics were done using SPSS software (Statistical Package for the Social
Sciences, version 11.0, SSPS Inc, Chicago, Ill, USA).
Results
Age and Symptom Frequency
The average age for the 30 patients was 51.33 years, (range, 26–76 years; SD
14.19). Symptoms most commonly recorded in the patients’ charts were obstructive urinary symptoms (80%), pain (73%), sexual dysfunction (70%), and irritative urinary symptoms (60%) (Table 1).
Table 1 . Symptoms recorded in the charts of 30 men with chronic urogenital complaints.
Symptom Score Changes During Treatment
For all 30 patients, the average global symptom severity score dropped from a mean of 6.40 (range, 3-10; SD, 2.04) at the first visit to a mean of 1.95 (range, 0-
9; SD, 2.25) at the last visit, a reduction of 69.53%, which was statistically significant (mean difference, 4.44; CI, 3.37 – 5.52); t(29) = 8.47; P < 0.0001) (Table 2).
Table 2 . Symptom scores for 30 men. V = visit. First, peak, and last symptom scores are shown as well as all data points for each patient.
Symptom score peaks tended to occur at the beginning of treatment (Figure 1).
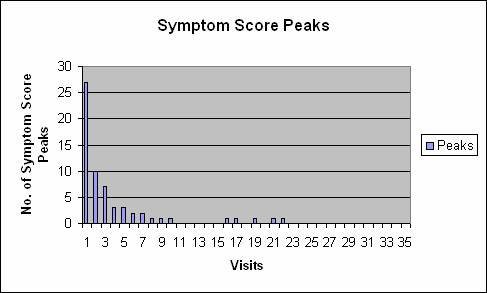
Figure 1 . Symptom score peaks in 30 men. Twenty-nine of 30 men had their first symptom score peak at the first or second visit. All symptom score peaks are graphed.
Symptoms Scores in 10 Men Versus 20 Men
Ten of the 30 patients (33%; mean age, 51.00 years; range, 26–72 years; SD
14.60) reported complete remission of their symptoms by their last clinic visit. Their average symptom score dropped from 6.60 (range, 3-10; SD, 2.59) at the beginning of treatment to 0.00 at the end, which was significant (mean difference,
6.60; CI, 4.75 – 8.45; t(9) = 8.06; P < .0001).
Twenty of the 30 men (67%; mean age, 51.50 years; range, 26–76 years; SD,
14.36) did not report complete remission of symptoms. In this group of 20 men, the mean first symptom score of 6.30 (range, 3–10; SD, 1.78) declined to a mean last symptom score of 2.93 (range, 0.10-9.00; SD 2.17), which was also significant (mean difference, 3.37; CI, 2.25 – 4.49; t(19) = 6.27; P < 0.0001).
Within this group of 20 men without complete remission of symptoms were 3 men (mean age, 47.33; range, 40–62 years; SD, 12.70) who reported not being any better at the end of treatment. Two of these 3 men reported the same symptom score at the beginning of treatment as at the end of treatment, and in 1 of the 3 men, the symptom score was higher at the end of therapy than it was at the start of therapy. In these 3 men, the mean symptom score rose from 6.67 (range, 6-8; SD, 1.15) at the beginning of treatment to 7.00 (range, 6-9; SD, 1.73) at the end
of treatment.
Our graph shows the mean first symptom score, the mean peak symptom score, and the mean last symptom score of the 10 men reporting complete remission of
symptoms versus the 20 men not reporting complete remission of symptoms
(Figure 2).
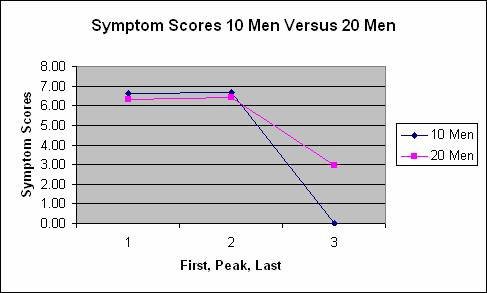
Figure 2 . Graph of the mean first, peak, and last symptom scores in 10 men reporting complete remission of symptoms versus 20 men not reporting complete remission of symptoms.
Urethral Bacteria
Smears of the urethral tip were collected 514 times in the 30 men (mean, 17.13;
range, 10-35; SD, 4.80).
Bacteria were present in 28 of 30 (93%) of the men’s Gram-stained urethral smears during treatment. By the last examination, bacteria were present in only 6 of the 30 (20%) Gram-stained urethral smears. Gram-positive bacteria were seen in urethral Gram-stains more often than were Gram-negative bacteria (Table 3).
Table 3 . The presence of bacteria in the urethral Gram-stains of 30 men.
Urethral WBCs
Urethral WBC counts declined to zero over time in all 30 men (Table 4).
Table 4 . Urethral WBC counts, first, peak, and last, and all data points in 30 men.
We performed Friedman’s test to test for differences between the first, peak, and last urethral WBC counts in the 30 men and the test was significant (P < 0.0001). The mean urethral WBC counts are tabulated (Table 5).

Table 5 . Mean first, peak, and last urethral WBC counts in 30 men.
Using the Wilcoxon signed ranks test and our Bonferroni correction of less than
0.017 being significant, we then compared paired groups of data. The difference between the first urethral WBC counts (mean, 3.07; median, 0.00) and the peak (mean, 6.93; median, 1.50) was significant (P = 0.003). The difference between the peak (mean, 6.93; median, 1.50) and the last (mean, 0.00; median, 0.00) was significant (P < 0.0001). In addition, the difference between the first group (mean,
3.07; median 0.00) and the last group (mean, 0.00; median 0.00) was significant
(P = 0.012).
Urethral WBC Peaks
Urethral WBC counts tended to peak early during therapy. Sixteen men had microscopic urethral purulence during therapy. Fourteen of the 17 urethral WBC peaks occurred during the first 5 specimen collections (Figure 3).
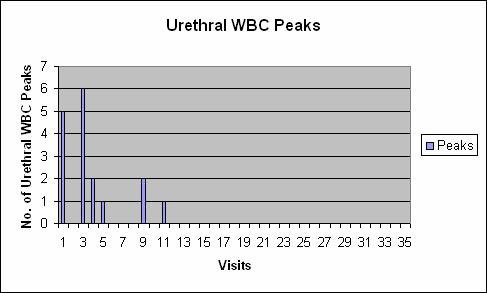
Figure 3 . All urethral WBC peaks are graphed. Fourteen of the 17 (82.35%)
urethral WBC peaks occurred during the patients’ first 5 clinic visits.
Urethral WBCs: 10 Men Versus 20 Men
We graphed the mean first, peak, and last urethral WBC counts of the 10 men who reported a complete remission of symptoms versus the 20 men who did not report a complete remission of symptoms (Figure 4).
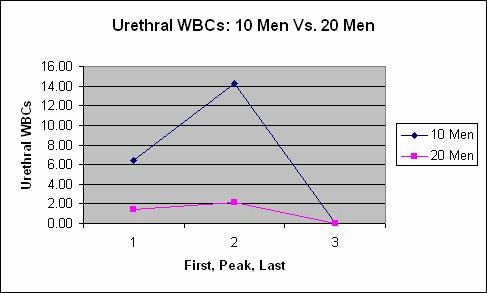
Figure 4 . Mean first, peak, last, urethral WBC counts in 10 men with complete remission of symptoms versus 20 men without complete remission of symptoms.
We also tabulated the mean and median urethral WBC counts in the 10 men who underwent a complete remission of symptoms versus the 20 men who did not undergo a complete remission of symptoms to demonstrate that the urethral fluid from the 10 men was more purulent at the first and peak specimens than that of the 20 men (Table 6).
Table 6 . Mean and median first, peak, and last urethral WBC counts in 10 men with a complete remission of symptoms versus 20 men without complete remission of symptoms.
We used the Mann-Whitney test to compare the first urethral WBC counts in 10 men who underwent complete remission versus the first urethral WBC counts in
20 men who did not undergo complete remission, and the difference did not reach significance (P = 0.553). We compared the peak urethral WBC counts in
10 men versus the peak urethral WBC counts in 20 men, and the difference was significant (P = 0.015). There was no difference in the last values between the 2
groups as all values were zero.
Urethral RBCs
The urethral smears were examined for RBCs, but they were seen only once during the 514 urethral smear examinations, at the first clinic visit, in patient No.
12. All urethral RBC counts were zero at all other times, which demonstrates that our technique is not traumatic. Chlamydia trachomatis
Eight of the 30 men had fluorescing C. trachomatis elementary bodies by (direct fluorescent antibody) DFA at their first visit. Eight more men showed fluorescing C. trachomatis elementary bodies at a later DFA test during the protocol; overall,
16 of the 30 men (53.33%) showed fluorescing C. trachomatis elementary bodies. Fifteen of the 16 Chlamydia positive men had fluorescing C. trachomatis elementary bodies seenduring their first or second visit. Fourteen of the 16 (87.50%) men with fluorescing C. trachomatis elementary bodies had a negative C. trachomatis DFA recorded in their charts prior to discharge from the treatment protocol (Table 7).
Table 7 . Number of fluorescing C. trachomatis elementary bodies seen at each test that was performed. Only patient No. 8 did not undergo at least 1 Chlamydia DFA test.
Urethral WBCs Versus Chlamydia
Of the 16 men with fluorescing C. trachomatis elementary bodies, 10 (62.5%) had urethral WBCs at some point during the treatment period, while 6 (42.85%) did not display urethral purulence at any time during treatment.
The C. trachomatis DFA testing was not performed at standard intervals, so we make no strong conclusions. We noted; however, that in the 10 patients in this study who reported complete remission of symptoms, 9 had 1 or more fluorescing C. trachomatis elementary bodies, and in 8 of those 9 patients, a repeat DFA test documented that fluorescing C. trachomatis elementary bodies had disappeared. Doing only 1 DFA test would have missed finding 7 patients with fluorescing Chlamydia elementary bodies.
Urethral Yeast
Five patients (Nos. 2, 10, 11, 26, and 30) had yeast reported in their urethral smears at some point by microscopy. Expressed
Prostatic Secretions (EPS)
Prostatic massage with expressed prostatic secretions (EPS) collection was performed 514 times in the 30 men (mean, 17.13; range, 10-35; SD, 4.80).
The Gram-stains of the EPS revealed visible bacteria by light microscopy in only
3 (10%) men (patients No. 12, 19, and 26). All three of these men also demonstrated fluorescing C. trachomatis elementary bodies (Table 8).
Table 8 . EPS Gram-stain results for the 3 men who had findings are tabulated, along with first and last symptom scores. GNB = Gram-negative bacilli, GNCoB = Gram-negative coccobacilli, GPC = Gram-positive cocci, GPB = Gram-positive bacilli.
Patient No. 19, who had multiple bacteria seen by Gram-staining his EPS, only dropped in symptom score from 5 at the beginning of treatment to 4 at the end of treatment, while patients Nos. 12 and 26 responded well to treatment.
EPS WBC Counts in the 30 Men
The mean EPS white blood cell counts for the 30 men demonstrated a rise and fall during treatment (Table 9).
Table 9 . EPS WBC counts in the 30 men. First, peak, and last values are listed, followed by all data points.
Friedman’s test revealed a significant difference between the first, peak, and last EPS WBC counts in the 30 men (P < 0.0001). Using the Wilcoxon signed ranks test with our Bonferroni correction of P less than 0.017 being significant, the first EPS WBC counts (mean, 12.40; median, 6.00) and the peak EPS WBC counts (mean, 36.50; median, 39.00) were significantly different (P = 0.0001). The peak EPS WBC counts (mean, 36.50; median, 39.00) and the last EPS WBC counts (mean, 10.53; median, 6.50) were also significantly different (P = 0.0001). The difference between the first and last EPS WBC groups did not reach significance (P = 0.810) (Table 10).

Table 10 . The mean, range, standard deviation, and median first, peak, and last
EPS WBC counts.
The rise and fall of EPS WBC counts demonstrates that the clinical horizon exists and suggests that obstructed prostatic acini are being drained during treatment.
EPS WBC Peaks
When examining the EPS WBC counts under 1000X microscropy, 17 of the 30 (56.67%) men had 5 or more WBCs at their first massage, while 29 of the 30 men (96.67%) had an EPS WBC count of 5 or more by the eighth prostatic massage. Patient No. 8 was the only patient who did not have 5 or more WBCs in the EPS during the treatment period. Only 11 of the 30 men (36.67%) had an EPS WBC count over 10 at the first massage, while 26 of the 30 men (86.66%) had an EPS WBC count over 10 at some point during therapy. These results show that repetitive prostatic massage shifts most men into the classification of inflammatory prostatitis.
Only 3 of 30 men (10%) had their most elevated EPS WBC count at their first prostatic massage, while 6 of the 30 men (20.00%) peaked at the sixth massage. It took 6 massages per patient to achieve the EPS WBC peak in over 50% of the patients. None of the EPS WBC counts peaked at the last EPS collection in any of the men studied. These findings have important implications, and clearly show that many prostatic massages must be done to obtain the most purulent EPS specimen for disease classification and microbial testing (Figure 5).
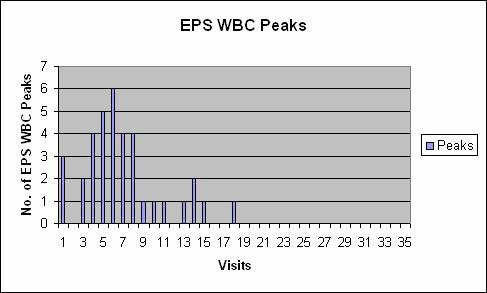
Figure 5 . All EPS WBC peaks are graphed. The highest number of peaks was at the sixth prostatic massage. Thirty of 36 (83.33%) of peaks occurred during the first 10 visits.
EPS WBCs: 10 Men Versus 20 Men
We graphed the mean EPS WBC counts for the 10 men who reported a complete remission of symptoms versus the 20 men who did not report a complete remission of symptoms (Figure 6).
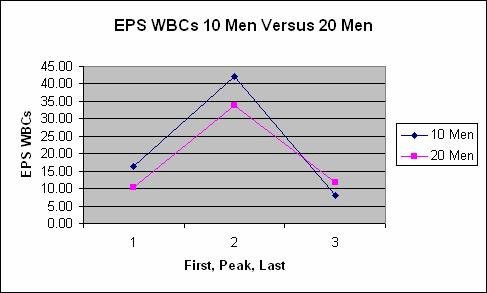
Figure 6 . Mean EPS WBCs in 10 men versus 20 men at the first, peak, and last visits.
We also tabulated the mean and median first, peak, and last EPS WBC counts for the 10 men who reported a complete remission of symptoms versus the 20 men who did not report a complete remission of symptoms(Table 11).
Table 11 . Mean with range and standard deviation, and median first, peak, and last EPS WBC counts in 10 men who reported complete remission of symptoms, versus 20 men who did not report complete remission of symptoms.
We used the Mann-Whitney test to determine if the first EPS WBC counts in 10 men differed from the first WBC counts in 20 men in a statistically significant fashion, and the difference did not reach significance (P = 0.102). The difference between the peak EPS WBC counts for the 10 men and the peak EPS WBCs counts for the 20 men also did not reach significance (P = 0.255). And finally, the difference between the last EPS WBC counts for 10 men and the last EPS WBC counts for 20 men did not reach significance (P = 0.508).
EPS WBC Counts versus Urethral WBC Counts
We compared mean EPS WBC counts at each visit with the urethral WBC counts at each visit, since both fluids were examined under 1000X magnification. The mean of the mean urethral WBC counts over 35 visits was 0.38 (range, 0.00–
4.07; SD, 0.96; median, 0.00) and the mean of the mean EPS WBC counts over
35 visits was 14.26 (range, 1–28; SD, 5.12; median, 14.53). The difference between the mean EPS WBC counts and the mean urethral WBC counts at each visit was significant (P < 0.0001). The EPS was significantly more purulent than the urethral smears.Urethral WBC Peaks versus EPS WBC Peaks
We compared the peak urethral WBC counts in the 16 men who had urethral WBCs present against the peak EPS WBC counts. The urethral WBC peaks tended to occur earlier than the EPS WBC peaks (Figure 7).
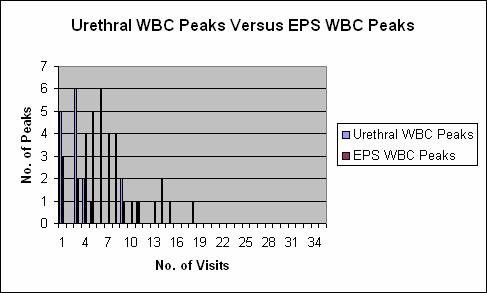
Figure 7. Urethral WBC peaks versus EPS WBC peaks. The peaks in urethral inflammation tended to occur earlier in therapy than EPS WBC peaks. All peaks are graphed.
EPS Red Blood Cells (RBCs)
We tabulated the EPS RBC counts in the 30 men, which went to zero over time in all 30 men (Table 12).
Table 12 . EPS red blood cells, first, peak, last, and all data points for the 30 men. EPS RBCs went to zero by the last visit in all patients.
We performed Friedman’s test to test for differences between the first, peak, and last EPS RBC counts, and a significant difference existed (P < 0.0001). We applied the Wilcoxon signed ranks test with our Bonferroni correction of P less than 0.017 as significant to compare paired groups. The difference between the
first EPS RBC counts (mean, 0.17; range, 0–5; SD, 0.91; median, 0.00) and the peak EPS RBC counts (mean, 4.10; range, 0–45; SD, 9.46; median, 0.00) was significant (P = 0.001). The difference between the peak EPS RBC counts (mean, 4.10; median; 0.00) and the last EPS RBC counts (mean, 0.00; median
0.00) was significant (P = 0.001). The difference between the first EPS RBC
counts (mean, 0.17; median 0.00) and the last EPS RBC counts (mean, 0.00, median 0.00) was not significant (P = 0.317), possibly due to small numbers.
EPS RBC Peaks Versus EPS WBC Peaks
We graphed the EPS WBC peaks and the EPS RBC peaks, and the peaks tended to overlap. All but one of the EPS RBC peaks occurred between the second to ninth visits, with the highest number of peaks occurring at the fifth and sixth massages (Figure 8).
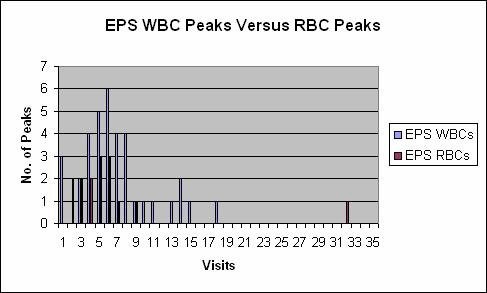
Figure 8. All EPS WBC peaks versus all EPS RBC peaks.
EPS RBCs: 10 Men Versus 20 Men
We graphed the mean EPS RBC counts at the first, peak, and last visits for the
10 men reporting a complete remission of symptoms versus the 20 men not reporting a complete remission of symptoms (Figure 9).
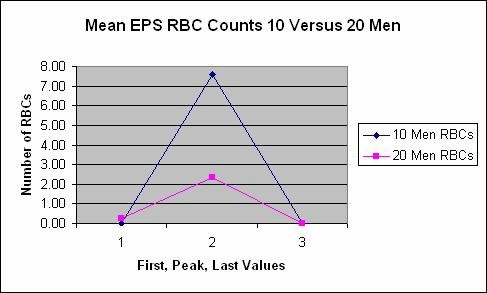
Figure 9. Mean first, peak, and last EPS RBC counts in 10 men reporting a complete remission of symptoms versus 20 men not reporting a complete remission of symptoms.
We also tabulated the mean and median first, peak, and last RBC counts in the
10 men who reported a complete remission of symptoms to compare with the 20 men who did not report a complete remission of symptoms (Table 13).
Table 13 . Mean, range, standard deviation, and median EPS WBC counts in 10 men reporting a complete remission of symptoms and the 20 men not reporting a complete remission of symptoms.
We used the Mann-Whitney test to compare the first EPS RBC counts in the 10 men versus the first EPS RBC counts in the 20 men and the difference was not significant (P = 0.48). The difference between the peak EPS RBC counts in the
10 men versus the peak EPS RBC counts in the 20 men also did not reach significance (P = 0.592). The last EPS RBC values were all zero in both groups.
EPS Yeast
Patient No. 11 was the only patient to have yeast seen in his EPS during treatment. He was one of the 10 patients who reported complete remission of symptoms.
EPS Cultures
All patients had a complete set of EPS cultures done on their first EPS specimen. EPS cultures were sometimes repeated during treatment, especially if the EPS WBC count rose during treatment. Staphylococcus species were most commonly cultured. One patient, patient No. 9, was positive for Ureaplasma (Table 14).
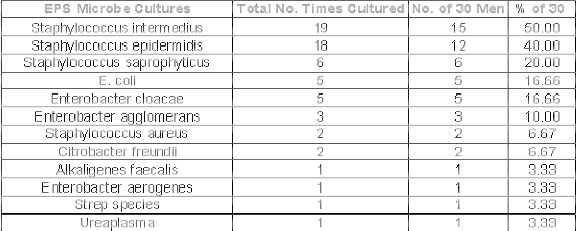
Table 14 . EPS WBC culture results in 30 men with chronic urogenital complaints.
We compared the 5 men who were E. coli positive (patients Nos. 7, 11, 14, 25, and 26) with the 25 who were E. coli negative for descriptive purposes. We noted that the 5 men who were E. coli positive were less likely to have as great an improvement in symptom scores over time, were less likely to have urethral inflammation, had lower mean first EPS WBC values, were not associated with EPS RBCs, and had lower peaks in post-massage urinary WBCs.
Urine Results
Post-massage urine samples were obtained 514 times in the 30 men (mean,
17.13; range, 10–35; SD, 4.80). We tabulated the urinary WBCs (Table 15).
Table 15 . Urinary WBC counts, first, peak, last, and all data points for the 30 men.
We tabulated the mean and median values for the urinary WBC counts in the 30 men (Table 16).

Table 16 . Mean, range, standard deviation, and median first, peak, and last urinary WBC counts in the 30 men.
The Friedman test was significant for differences between the first, last, and peak urinary WBC counts in the 30 men (P < .0001). We applied the Wilcoxon signed ranks test using our Bonferonni correction of P less than 0.017 being significant
to compare the pairs of groups. The difference between the first urinary WBC
counts (mean, 10.63; median, 4.00) and the peak urinary WBC counts (mean,
30.73; median 25.00) was significant (P < 0.0001). The difference between the peak urinary WBC counts (mean, 30.73; median, 25.00) and the last urinary
WBC counts (mean, 6.93; median, 3.00) was also significant (P < .0001). The
difference between the first urinary WBC counts (mean, 10.60; median, 4.00) and the last urinary WBC counts (mean, 6.93; median 3.00) did not reach significance (P = 0.855).
Urine WBC Peaks
We graphed all the urinary WBC peaks in the 30 men along with the EPS WBC peaks, and our graph demonstrates a temporal relationship between the EPS and urinary WBC peaks, indicating that the post-massage urine does, to some degree, reflect the EPS (Figure 10).
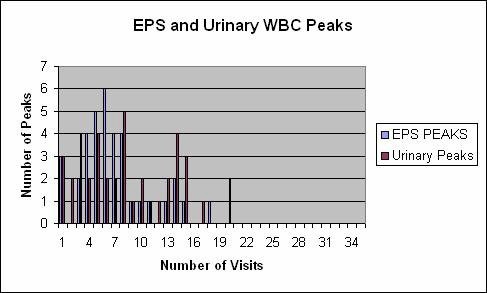
Figure 10. EPS and Urinary WBC peaks in 30 men. All peaks are graphed.
Urinary WBCs: 10 Men Versus 20 Men
We graphed the urinary WBC counts of the 10 men who reported complete remission of symptoms versus the 20 men who did not report complete remission of symptoms. The mean first and peak urinary WBC counts were higher in the men who underwent complete remission of symptoms (Figure 11).

Figure 11. Mean urine WBC counts, first, peak, and last, in 10 men with complete remission of symptoms versus 20 men without complete remission of symptoms.
We tabulated the mean and median urinary WBC counts for the 10 men who underwent a complete remission of symptoms as well as for the 20 men who did not report undergoing a complete remission of symptoms (Table 17).
Table 17 7. Mean, range, standard deviation, and median first, peak, and last urinary WBC counts in 10 men who underwent a complete remission of symptoms versus 20 men who did not undergo a complete remission of symptoms.
We used the Mann-Whitney test to compare whether the first post-massage urinary WBC counts in the 10 men who reported a complete remission of symptoms (mean, 16.90; median, 6.50) differed from the first post-massage urinary WBC counts in 20 men who did not report a complete remission of symptoms (mean, 7.45; median, 3.00) and the difference was significant (P =
0.032). We compared the peak urine WBC counts in 10 men (mean, 32.00;
median, 30.00) to the peak urine WBC counts in 20 men (mean, 30.10; median,
25.00) and the difference was not significant (P = 0.642). We also compared the last urine WBC counts in 10 men (mean, 13.20; median 6.50) versus the last
urine WBC counts in 20 men (mean, 3.80; median, 3.00) and the difference did not reach significance (P = 0.184).
Urinary RBCs
We tabulated the post-massage urinary RBC counts for the 30 men (Table 18).
Table 18. Urinary RBCs, first, peak, last, and all data points for the 30 men.
We performed the Friedman test for differences between the first, peak, and last post-massage urinary RBC counts, and a significant difference was present (P <
0.0001) (Table 19).

Table 19. Mean and median, first, peak, and last post-massage urinary RBC
counts.
We applied the Wilcoxon signed ranks test with our Bonferroni correction of P less than 0.017 being significant to compare paired groups. The difference between the first post-massage urinary WBC counts (mean, 2.97; median, 2.00) and the peak post-massage urinary RBC counts (mean, 9.70; median, 6.00) was significant (P < 0.0001). The peak urinary RBC counts (mean, 9.70; median,
6.00) and the last urinary RBC counts (mean, 2.03; median, 1.00) were also significantly different (P < 0.0001). The difference between the first urinary RBC counts (mean, 2.97; median, 2.00) and the last (mean, 2.03; 1.00) was not significant (P = 0.069).
Urinary RBCs: 10 Men Versus 20 Men
We graphed the mean post-massage urinary RBCs at the first, peak, and last visits for the 10 men reporting a complete remission of symptoms versus the 20 men not reporting a complete remission of symptoms (Figure 12).
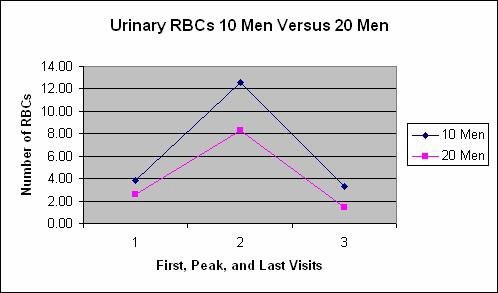
Figure 18 . Mean urinary RBCs in 10 men reporting a complete remission of symptoms versus 20 men not reporting a complete remission of symptoms.
We also tabulated the mean and median urinary RBCs for the 10 men who reported a complete resolution of symptoms and for the 20 men who did not report a complete resolution of symptoms, and noted that in the group of 10 men the post-massage urine mean and median RBC counts were higher than in the group of 20 men (Table 20).
Table 20. Mean, range, standard deviation, and median urinary RBC counts in 10 men versus 20 men.
We used the Mann-Whitney test to look for differences between the RBC counts in the group of 10 men versus the group of 20 men. We compared the first RBC counts in 10 men (mean, 3.80; median, 3.00) to the first RBC counts in 20 men (mean, 2.55; median, 1.50) and the difference was not significant P = 0.360). We compared the peak RBC counts in 10 men (mean, 12.60; median, 8.00) versus the peak RBC counts in 20 men (mean, 8.25; median, 6.00) and the difference was not significant P = 0.278). And, we compared the last RBC count in the 10 men (mean, 3.30; median, 1.50) versus the last RBC count in the 20 men (mean,
1.40; median, 1.00), and the difference was not significant (P = 0.469).
Urinary Trichomonas
Trichomonas was seen in the first post-massage urine of 2 patients (patient Nos.
1 and 27).
Urinary Yeast
Five patients (patient Nos. 1, 10, 11, 25, and 26) had yeast seen in their post- massage urine. Overall, 7 of the 30 men in this study (patient Nos. 1, 2, 10, 11,
25, 26, 30) were reported, by microscopy, to be positive for yeast in their urethral smears, prostatic fluid, or post-massage urine. In the 7 yeast-positive patients, the mean first symptom score was 7.57 (range, 5-10; SD, 2.5). The mean last symptom score was 3.47 (range, 0-9; SD, 3.47). The decline in symptom scores from first to last was significant (P = 0.033). Four of the 7 yeast-positive patients
were in the group of 10 men with complete remission of symptoms.Antimicrobials
Prescribed for the 30 Men
We list all the medications prescribed to the patients and their frequency of use. All 30 patients were prescribed either doxycycline or minocycline. Twenty-eight of
30 men (93.33%) were prescribed metronidazole. Twenty-eight of 30 men (93.33%) were prescribed antifungals, and many were prescribed both fluconazole and itraconazole. Patients No. 9 and No. 17 were not prescribed antifungals and neither tested positive for yeast during treatment. Cefixime, ofloxacin, and azithromycin were also prescribed frequently. Three patients took the herb, Pygeum africanum, on their own during the study (Table 21).
Table 19 1. Antimicrobials and other medications prescribed to the 30 men and frequency of use. Pygeum africanum use is also noted.
Comparing 10 Men Versus 20 Men
For additional gross descriptive purposes we again divided the 30 men into two groups: the 10 men reporting a complete resolution of symptoms and the 20 men who did not report a complete resolution of symptoms (Table 22).
Table 20 2. Frequency table of 10 men versus 20 men showing age, number of massages, symptom scores, and urethral WBCs.
We noted that both groups had the same frequency of being positive for WBCs in the urethra at the first visit (30%); however, in the group of 10 men with complete remission, 80% showed urethral WBCs at some point during therapy, while the group of 20 men showed urethral WBCs only 30% of the time.
Cell Counts: 10 Men Versus 20 Men
We tabulated the mean and median WBC and RBC counts for the 10 men reporting a complete remission of symptoms versus the 20 men not reporting a complete remission of symptoms (Table 23).
Table 21 . Mean WBC counts in different fluids and in 30 men, 10 men, 20 men, and 3 men.
In the 10 men who underwent complete remission of symptoms, the mean and median EPS WBC counts fell from first to last. This contrasts with the 20 men who did not have complete remission, where the mean and median EPS WBC counts rose from first to last. In almost all cases the first and peak cell counts were higher in the 10 men who underwent complete remission of symptoms than in the 20 men who did not report a complete remission of symptoms.
Microbial Diagnosis
For descriptive purposes, we made a frequency table of all the microbes diagnosed during treatment in 10 men reporting complete resolution of symptoms versus the 20 men not reporting complete resolution of symptoms (Table 24).
| Frequency Table | 10 Men | % of10 | 20Men | %of20 |
| Chlamydia | ||||
| Chlamvdia Fluorescinq EBs | 9.00 | 90.00 | 7.00 | 35.00 |
|
Chlamvdia DFA neoative at end RX |
8.00 |
80.00 |
6.00 |
30.00 |
|
Urethral Bacteria |
||||
|
Gram-positive cocci |
9.00 |
90.00 |
18.00 |
90.00 |
|
Gram-negative diplococcus |
1.00 |
10.00 |
1.00 |
5.00 |
|
Gram-negative minute cocci |
3.00 |
30.00 |
5.00 |
25.00 |
|
Gram-positive bacilli |
3.00 |
30.00 |
10.00 |
50.00 |
|
Gram-negative bacilli |
1.00 |
10.00 |
4.00 |
20.00 |
|
Gram-negative coccobacilli |
0.00 |
0.00 |
4.00 |
20.00 |
|
EPS Bacteria |
||||
|
Gram-neoative bacillus |
1.00 |
10.00 |
0.00 |
0.00 |
|
I Gram-neoative coccobaciIIus |
0.00 |
0.00 |
1.00 |
5.00 |
|
I Gram-positive cocci |
0.00 |
0.00 |
2.00 |
10.00 |
|
I Gram-positive bacillus |
0.00 |
0.00 |
1.00 |
5.00 |
|
VB3 Bacteria |
||||
|
present |
0.00 |
0.00 |
0.00 |
0.00 |
|
EPS Microbe Cultures |
||||
|
Staphvlococcus epidermidis |
5.00 |
50.00 |
13.00 |
65.00 |
|
Staphvlococcus intermedius |
5.00 |
50.00 |
14.00 |
7000 |
|
Staphvlococcus saprophvticus |
2.00 |
20.00 |
4.00 |
20.00 |
|
Staphvlococcus aureus |
2.00 |
20.00 |
0.00 |
0.00 |
|
E. coli |
1.00 |
10.00 |
4.00 |
20.00 |
|
Enterobacter cloacae |
0.00 |
0.00 |
5.00 |
25.00 |
|
Enterobacter aqqlomerans |
1.00 |
10.00 |
2.00 |
10.00 |
|
Alcalioenes faecalis |
1.00 |
10.00 |
0.00 |
0.00 |
|
Citrobacter freundii |
0.00 |
0.00 |
1.00 |
5.00 |
|
Enterobacter aerooenes |
0.00 |
0.00 |
1.00 |
5.00 |
|
Strep species |
1.00 |
10.00 |
0.00 |
0.00 |
|
Summary EPS Microbe Cultures |
||||
|
Men with EPS Gram-positives |
8.00 |
80.00 |
17.00 |
85.00 |
|
Men with EPS Gram-negatives |
3.00 |
30.00 |
11.00 |
55.00 |
|
Ureaplasma/Mycoplasma |
||||
|
I Ureaplasma |
0.00 |
0.00 |
1.00 |
5.00 |
|
Yeast discovered |
||||
|
yeast in EPS |
1.00 |
10.00 |
0.00 |
0.00 |
|
yeast in urethra |
3.00 |
30.00 |
1.00 |
5.00 |
|
yeast in post-massage urine |
2.00 |
20.00 |
3.00 |
15.00 |
|
Yeast Summary |
||||
|
Yeast found anvwhere |
4.00 |
40.00 |
3.00 |
15.00 |
|
Trichomonas |
||||
|
Trichomonas in post-massage urine |
0.00 |
0.00 |
2.00 |
10.00 |
Table 22 4. Microbes diagnosed and frequency of diagnoses during therapy in 10 men versus 20 men.
In the 10 men reporting complete remission of symptoms, 90% were positive for fluorescing C. trachomatis elementary bodies, and 80% had a negative DFA test before treatment ended (1 patient was not retested at the end of therapy). Of the
20 men without complete remission, only 35% had fluorescing C. trachomatis
elementary bodies seen, and only 30% had a negative test result documented before the end of therapy.
The 10 men with complete remission of symptoms were less likely to have Gram- negative bacteria seen in the EPS, and were more likely to have yeast seen in their urethral smears, EPS, or urine than the other 20 men.
Antibiotic Therapy: 10 Men Versus 20 Men
For descriptive purposes, we tabulated the antibiotic therapy for the 10 men versus the 20 men (Table 25).
Table 23 5. Medication use and frequency in the 30 men.
The 10 men reporting complete remission of symptoms received minocycline, cefixime, and azithromycin at greater frequencies than the group of 20 men.
The table also lists the urologic medications given. Only 1 patient in the group of
10 men self-reporting complete remission of symptoms received a urologic medication. Patients who did not undergo complete remission were much more likely to receive alpha-blocker medication or finasteride. This makes sense, because when patients did not improve, the treating physicians often added urological medications.
The 3 patients who took Pygeum africanum on their own did not have an improved remission rate.
Transrectal Ultrasound (TRUS)
Patient No. 1 in this study was the only patient to have a transrectal ultrasound (TRUS) before and after treatment. His presenting prostate size was 41 grams, while his TRUS measured 27 grams after completing therapy, a decline in size of
34.14%. Previously, we published a paper in which the size of a 78-year-old man’s prostate declined in size by 52%, from 63 g to 30 g, after repetitive prostate massage and antimicrobial therapy.[4] Another paper pending
publication (Hennenfent BR, Lazarte AR, and Feliciano Jr. AE: Five Men in Acute Urinary Retention Spared Transurethral Resection of the Prostate by Repetitive Prostatic Massage and Medical Therapy) reports decreased TRUS-measured prostate size after repetitive prostatic massage and antibiotic therapy in two men.
Discussion
Since the 1970s, Manila physicians have been treating prostatitis as an infection and obstruction of the prostate, using repetitive prostatic massage to completely drain the prostate, along with microbial diagnosis, and antimicrobial therapy. Most of the men in this study, in the clinical judgment of the treating physicians, were suffering from chronic prostatitis or benign prostatic hyperplasia (BPH) with chronic prostatitis.
In the medical literature, repetitive prostatic massage combined with microbial diagnosis and antimicrobial therapy, has achieved success in terms of patient- reported improvement of symptoms for patients with chronic prostatitis and chronic refractory prostatitis.
In 1998, we reported on 3 American men with chronic prostatitis, refractory to treatment in the United States, who were treated at the Manila Genitourinary Clinic with 19, 27,and 21 prostatic massages respectively. The men also underwent microbial diagnosis and received antimicrobial therapy. All three men reported undergoing complete remission of their symptoms. At last follow-up at
29 months, 26 months, and 15 months, respectively, all men were asymptomatic.[5]
In 1998, an article was published about a 69-year-old man who presented to Antonio Novak Feliciano’s clinic (Makati, Philippines) with acute urinary obstruction wearing an indwelling urinary catheter. He had been diagnosed with BPH by an urologist and had been told he needed to undergo transurethral resection of the prostate. He also complained of impotence, having had no erection for many years. The catheter was removed, the man was treated with 8 prostatic massages, microbial tests were done, and antibiotics were given. The man reported that his urinary symptoms completely resolved and his sexual function returned by 60% – 70%. At last follow-up, the man had avoided surgery for over 5 years, and at 5 years reported normal urination with only occasional nocturia. [6]
In 1998, we reported on 35 men, average age 45 years, with chronic urogenital complaints who were treated with repetitive prostatic massage and antimicrobial therapy. Their EPS was examined a total of 347 times. Five of the patients could be reached for long-term follow-up and 4 of those 5 patients reported complete remission of symptoms, with the fifth patient, who had diabetes mellitus, reporting continuing sexual dysfunction.[7]
In 1999, in collaboration, we published a prospective study of men with chronic refractory prostatitis who had been to many previous physicians, and had already received multiple rounds of antibiotics. Some of these men had undergone surgery and other procedures, and many of them had been sick for years or decades. Twenty-two men entered treatment. Average follow-up was 17 months. Five of the 22 patients (23%) had complete remission of symptoms, and overall, based on Subjective Global Assessment scores, 66.6 percent of the patients experienced marked, moderate, or mild improvement of their chronic
prostatitis.[8]
In 1999, independent of the previous studies, a study was published of 73 men with chronic prostatitis who were treated with repetitive prostatic massage and antibiotic therapy. The average age of the men was 43.5 years, and the average duration of symptoms was 6.7 years. Overall, 40 percent of the patients underwent complete sustained remission of symptoms, 19 percent underwent complete remission followed by symptom recurrence, 21 percent experienced some improvement, and 21 percent had no improvement.[9]
Definitions of Prostatitis and Chronic Pelvic Pain Syndrome
Definitions of prostatitis and chronic pelvic pain syndrome are evolving.[10] The National Institutes of Health uses 10 or more WBCs per 400-power magnification as its inflammatory requirement for chronic pelvic pain syndrome; however, the National Institutes of Health criteria do not include repetitive prostatic massage. Schaeffer et al. (Chicago) examined prostatic fluid specimens at high power under a cover slip.[11] The Giessen group (Germany) uses 10 or more
leukocytes per 1000-power magnification in the EPS or VB3, after Papanicolaou
staining as their definition of inflammatory prostatitis.[12] Krieger et al’s work supports the belief that the Gram-stain is a conservative way to count EPS WBCs.[13]
In the current study, 17 of the 30 (56.67%) men had an EPS WBC count of 5 or more based on their first massage. Using all the massages to classify men, 29 of
30 (96.67%) men displayed an EPS WBC count of 5 or more at some point during EPS collection.
Eleven of the 30 (36.67%) men in this study had an EPS WBC count of 10 or more at the first massage, while 26 of the 30 men (86.67%) had an EPS WBC count over 10 at some point during the study.
The 1 patient who did not have 5 or more WBCs in the EPS under 1000X power, patient No. 18, was a 31-year-old man complaining of pelvic pain, irritative
urinary symptoms, and obstructive urinary symptoms, whose peak EPS WBC count never rose above 2 WBCs per 1000X, and last EPS WBC was zero. His symptom score dropped from 5 to 2.5 during the course of treatment, but it’s doubtful that he had inflammatory prostatitis.
The 10 men who underwent complete remission of symptoms all had an EPS WBC peak over 15 at some point during their EPS collections. In fact, the mean peak EPS WBC count in the 10 men was 42.00 (range, 15–60; SD 18.59; median, 45.00). The mean peak EPS WBC count in the 20 men who did not report complete resolution of symptoms was 33.75 (range, 2–60; SD, 22.10; median, 36.50). However, as noted earlier this difference did not reach significance (P = 0.255).
Men 50 Years of Age or Older
Because 18 of the 30 patients (60%) were 50 years of age or older, these 18 might have been diagnosed as having BPH by the typical urologist. All 18 patients aged 50 years and older (average age, 61.11 years) had prostatitis by a count of 5 or more WBCs in the EPS, and all 18 such patients also had 10 or more EPS WBCs at some point during therapy. Six of the 18 men aged 50 and older reported complete remission of symptoms; in fact, the average symptom score for these men dropped from 5.78 at the beginning of treatment to 1.51 at the end of treatment (P = 0.00029). The mean peak EPS WBC count in men aged 50 years or older was 41.22 (range 10–60, SD 19.51). We believe that failure to diagnose prostatitis in patients with BPH is a major problem with urological workups, as none of the men over age 50 who presented to the clinic with a diagnosis of BPH had been tested for prostatitis.Definition of Urethritis
The definition and diagnosis of urethritis is also evolving.[14] There is no clear definition of chronic urethritis, as opposed to acute urethritis. None of the patients in this study complained of urethral discharge, while 8 of 30 (26.66%) had a
urethral WBC count greater than 0 at their first urethral examination. Three of these men (30%) were in the eventual complete clinical remission group and 5 (25%) were not. Overall, 16 of 30 men (53.33%) were positive for urethral WBCs before treatment ended. This is similar to the National Institutes of Health cohort study, where urethral leukocytosis, defined as 1 or more WBCs in the first voided urine, was found in 243 of 488 cases (49.80%);[15] however, no tests for Chlamydia were done in the NIH study.
In our study, 8 of the 10 men (80%) in the complete remission group had urethral WBCs at some point during treatment. The mean peak EPS WBC count in the 8 men presenting with urethral pus at their first visit was 33.50 (range 5.00-60.00, SD 20.81).
The mean peak urethral WBC count in all 16 men who had urethral pus at some point during treatment was 41.44 (range 5–60, SD 19.93).
The mean peak EPS WBC count in the 14 men who never tested positive for
Chlamydia by DFA was 30.86 (range, 2-60; SD, 21.57).
Prostatic Massage Is Not Traumatic
It has been hypothesized that repetitive prostatic massage might cause trauma to the prostate. We looked at this by following the RBC counts in the EPS. The data show that while RBCs might be present at the first massage, or during the first several massages, EPS RBCs disappear during therapy. This finding has been consistent in our studies,[16,17] and we believe the improvement in RBC counts demonstrates that prostatic massage is therapeutic rather than traumatic. The occurrence of the WBC peaks and RBC peaks at the same times during the course of massages also serves to indicate that EPS RBCs reflect the inflammation of the prostate.
Prostatic Massages and Classification
We believe that repetitive prostatic massage and repetitive EPS collection is critical to the diagnosis and treatment of prostatitis and BPH. In this study, some men might have been classified differently using prostatitis/prostatodynia criteria or the chronic pelvic pain syndrome classification if repetitive prostatic massage had not been performed. Some men would have undergone surgical treatment for BPH instead of medical treatment for chronic prostatitis in others’ hands. We believe that our body of work strongly suggests that a one-time examination of the prostatic fluid is insufficient. Only 3 of 30 men (10%) had their highest EPS white blood cell count at their first massage, indicating that several prostatic massages must be done to obtain the most purulent specimen for disease classification and microbial testing.
We were able to obtain EPS in 100 percent of attempts in the 30 men studied, which compares favorably with the National Institutes of Health cohort study, where cohort physicians were only able to obtain EPS in 397 of 488 men (81.35%).[18] The failure of the cohort study to obtain EPS in almost 19% of men (91 of 488 men) puts all their study conclusions in jeopardy, as does basing all their classifications on a 1-time EPS collection. We believe that our ability to obtain EPS in 100 percent of patients over several studies is due to our
technique, which is designed to drain the prostate completely of all fluids, and our years of experience doing multiple massages per patient instead of a 1-time massage. A previous study reported that prostatic massage is a poorly studied procedure, and that patients perceive that physicians perform the procedure differently and only sometimes effectively.[19]
Obstruction
Besides obtaining fluid for classification and microbial diagnosis, our WBC count analyses in this paper, and previous papers, and our clinical findings suggest that repetitive prostatic massage unplugs the prostate. This is consistent with work by John W. Polacheck, M.D., and L. Eduardo Vega M.D. (A Beneficial Effect of Prostate Massage for Patients with Chronic Prostatits: The Expression of Intraglandular Prostatic Inflamatory Aggregates. Presented at the International Prostatitis Collaborative Network Third Annual Meeting, October 23-25, 2000, Arlington, Virginia). Indeed, as we noted earlier, we have documented TRUS- measured decreases in prostate size in some patients after repetitive prostatic massage. In addition, a recent paper demonstrated increased prostatic pressure, presumably from obstruction, and higher WBC counts in men with category IIIa chronic pelvic pain syndrome.[20]
We remind physicians of the age-old surgical caveat, which says that you must drain an infection to cure it. The mean EPS WBC and RBC counts rose and fell during treatment, which we believe demonstrates that obstructed pockets of purulence are released during the process of repetitive prostatic massage.
Leukocytes and Bacteria Counts Matter
One National Institutes of Health cohort study investigator writes: “Although men with CP routinely receive anti-inflammatory and antimicrobial therapy, recent studies suggest that leukocyte and bacterial counts do not correlate with severity of symptoms. These findings suggest that factors other than leucocytes and bacteria contribute to the symptoms associated with CPPS.”[21] However, our study, with statistically significant data, establishes relationships between declining WBC counts and improvements in patient-reported symptom scores. We also discovered that comparing men who reported a complete remission of symptoms versus men who did not report a complete remission of symptoms revealed significant differences in cell counts.
Other researchers have failed to see significant relationships with EPS WBC counts. One study reports: “In cases of abacterial prostatitis, neither the initial expressed prostatic secretion white blood count nor the presence of symptoms reliably predicted subsequent inflammation.”[22] We suggest that repetitive prostatic massage and multiple EPS WBC examinations are needed to see such relationships.
Chlamydia
Our study shows a relationship between fluorescing Chlamydia elementary bodies and symptom improvement, and suggests other possible microbial relationships. In contrast, the National Institutes of Health cohort study failed to test for Chlamydia despite the fact that 49.80% of the men in the study displayed urethral leukocytosis.[23] Treatment
By comparing the 10 men who underwent complete remission of symptoms by the end of therapy with the 20 men who did not report a complete remission of symptoms, we saw noteworthy associations. The most successful outcomes were in men whose EPS WBC counts declined the most; who were positive for C. trachomatis by DFA early in treatment; but whose C. trachomatis test turned negative by the end of treatment; and who were treated with metronidazole, cefixime, minocycline, and azithromycin. However, many antibiotics and antifungals were used, and it could have been other combinations that were important.
Retrospective Study
This study is a retrospective study with all the inherent flaws of such a study. For example, we encountered 12 instances of symptom scores not being documented; however, all the laboratory data on these patients were available. No post-treatment follow-up was performed because of lack of funding. This study also points out the need for a better method to quantify the number of
WBCs in specimens when they are too numerous to count under the microscope. A larger study than this one might have found more differences that would have reached statistical significance, and would have allowed more powerful subgroup analyses. More microbial tests, and other tests, could be added to our current protocol if cost were not prohibitive. This study has laid the groundwork for a larger study to be done, and we recommend prospective studies and randomized controlled studies when resources permit.Conclusions
Ninety percent (27 of 30) of men with chronic urogenital complaints improved during treatment with repetitive prostatic massage, antimicrobial therapy, and sometimes urologic medications; the mean global symptom severity score dropped from 6.40 (range, 3–10; SD, 2.04) at the first visit to 1.95 (range, 0–9; SD, 2.24) at the last visit, a 69.53% reduction, which was statistically significant
(mean difference, 4.44; 95% confidence interval [CI], 3.37–5.52); t(29) = 8.47; P
< 0.0001).
Ten of the 30 patients (33.33%) reported complete remission of their symptoms
by their last visit, their mean first symptom score dropping from 6.60 (range 3–10; SD, 2.59) to 0.00, which was also significant (mean difference, 6.60; CI, 4.75–
8.45; t(9) = 8.06; P < .0005).
Urethral Smears, expressed prostatic secretions, and post-massage urines were obtained 514 times from the 30 men. Importantly, EPS was obtained at every attempt (100% success rate).
The decline from the first urethral WBC count of 3.07 (range, 0–40; SD, 8.32) to the last of 0.00 was significant (P = 0.012).The decline from the mean peak urethral WBC count of 6.93 to the mean last value of 0.00 was also significant (P
< .0005). Thus, our painless, and non-traumatic, method of obtaining urethral smears provided statistically significant data about urethral WBC counts.
The rise from the mean first EPS WBC count of 12.40 (range, 0-60; SD, 15.91) to the mean peak EPS WBC count of 36.50 (range, 2–60; SD, 21.05) was
significant (P = 0.000006). The decline from the mean peak EPS WBC count of
36.50 to the mean last EPS WBC count of 10.53 (range, 0–54; SD, 11.60) was also significant (P = 0.000002). This data demonstrates the phenomenon of the clinical horizon, with the EPS WBC counts rising and then falling during therapy.
The decline of the mean peak EPS RBC count from 4.10 to the mean last value of 0.00 was significant (P = 0.001).
The decline of the mean peak post-massage urinary WBC count of 30.73 to the mean last post-massage urinary WBC count of 6.93 was significant (P < .0005). The decline of the mean peak post-massage urinary RBC count from 9.70 to the mean last count of 2.03 was also significant (P < .0005).
Fluorescing Chlamydia trachomatis elementary bodies were seen in 16 of 30 men (53.33%), and 14 of those 16 (87.50%) had a negative C. trachomatis DFA result recorded in their charts by the end of the treatment protocol. In the group of 10 men reporting complete clinical remission of symptoms, 9 had fluorescing C. trachomatis elementary bodies seen, and in 8 of those men the elementary bodies disappeared by the end of therapy (1 patient was not retested).
Repetitive prostatic massage to drain prostates of pus, combined with antimicrobial therapy directed against infection, results in a statistically significant improvement in symptom scores. The therapy also results in statistically significant improvements in WBC and RBC counts. We recommend that multiple specimens, not just 1, urethral, EPS, or post-massage urine specimen, be collected to obtain the most purulent specimens for microbial analysis and
disease classification. We describe a non-invasive method of obtaining urethral smears and we recommend Chlamydia testing. Importantly, our data showed that men who reported a complete remission of symptoms had statistically
significantly higher peak urethral WBC counts, higher peak EPS RBC counts,
and higher first post-massage urine WBC counts, than those who did not report a complete remission of symptoms.
Lastly, we believe that failure to diagnose prostatitis in patients with benign prostatic hyperplasia (BPH) is a major problem with urological workups, as none of the men over age 50 in this study who presented with a diagnosis of BPH had been tested for prostatitis.
Acknowledgements
The authors thank Steve Creech of Statistically Significant Consulting; Hazal Macadangdang, B.S. in statistics, University of the Philippines; Loyd Norella, M.D., MPHM; and Rena Pedaria for their help with statistics. We also thank physicians Bienvenido Garcia, M.D., and Alfred Lazarte, M.D.
This study was not funded, but the authors thank the Prostatitis Foundation (Prostatitis.org), a nonprofit organization devoted to publicizing and researching prostatitis.
Competing Interests
The author’s declare that they have no competing interests.Authors’ Contributions
BRH and AEF conceived the study. BRH managed the statistical analysis in consultation with others and wrote the paper. NEdV provided patient care, collected the data, and organized the data in a database. AEF provided overall clinical supervision of the project, provided direct patient care, and developed the clinical protocols.
All authors have read and approved the final manuscript.
References
[1]Hennenfent BR, Feliciano Jr. AE: Changes in white blood cell counts in men undergoing thrice-weekly prostatic massage, microbial diagnosis and antimicrobial therapy for genitourinary complaints. British Journal of Urology (1998):81,370-376.
[2] Gilroy CB, Thomas BJ, Taylor-Robinson D: Small numbers of Chlamydia trachomatis elementary bodies on slides detected by the polymerase chain reaction. J Clin Pathol. 1992
Jun;45(6):531-2.
[3] Meares EM, Stamey TA: Bacteriologic localization patterns in bacterial prostatitis and urethritis. Invest Urol. 1968 Mar;5(5):492-518.
[4] Hennenfent BR, Garcia BS, Feliciano Jr. AE: Symptom Improvement and Transrectal Ultrasound-Documented Reduction of Prostate Size after Repetitive Prostatic Massage and Antimicrobial Therapy. Journal of Pelvic Surgery. 8(5): 265-269; Sep 2002.
[5] Hennenfent BR, Feliciano Jr. AE: Clinical Remission of Chronic Refractory Pelvic Symptoms in Three Men. The Digital Urology Journal, July 24, 1998. Available at: http://www.duj.com/Article/Hennenfent1/Hennenfent.html
[6] Hennenfent BR and Feliciano AN: Release of Obstructive Prostatic Disease and Improvement of Erectile Dysfunction by Repetitive Prostatic Massage and Antimicrobial Therapy. The Digital Urology Journal October 5, 1998. Available at: http://www.duj.com/Article/Hennenfent2/Hennenfent2.html
[7] Hennenfent BR and Feliciano Jr. AE: Changes in white blood cell counts in Men undergoing thrice-weekly prostatic massage, microbial diagnosis, and antimicrobial therapy for genitourinary complaints. The British Journal of Urology, 1998;81:370-376.
[8] Nickel JC, Downey J, Feliciano Jr. AE, Hennenfent BR: Repetitive prostatic massage therapy for chronic refractory prostatitis: the Philippine experience.
Tech Urol. 1999 Sep;5(3):146-51.
[9] Shoskes DA and Zeitlin SI: Use of prostatic massage in combination with antibiotics in the treatment of chronic prostatitis. Prostate Cancer and Prostatic Diseases. May 1999, Volume 2, Number 3, Pages 159-162.
[10] Nickel JC, Nyberg LM, Hennenfent M. Research guidelines for chronic prostatitis: consensus report from the first National Institutes of Health International Prostatitis Collaborative Network. Urology. 1999 Aug;54(2):229-33.
[11] Wright ET, Chmiel JS, Grayhack JT, Schaeffer AJ. Prostatic fluid inflammation in prostatitis. J Urol. 1994 Dec; 152(6 Pt 2): 2300-3.
[12] Schneider H, Ludwig M, Hossain HM, Diemer T, Weidner W: The 2001 Giessen Cohort Study on patients with prostatitis syndrome–an evaluation of inflammatory status and search for microorganisms 10 years after a first analysis. Andrologia. 2003 Oct;35(5):258-62.
[13] Krieger JN, Ross SO, Deutsch LA, Fritsche TR, Riley DE. Counting leukocytes in expressed prostatic secretions from patients with chronic prostatitis/chronic pelvic pain syndrome. Urology. 2003 Jul;62(1):30-4.
[14] Gangaram HB, Akbal K, Gan AT, Hussein SH, Mangalam S, Rohani Y, Lai PF. Urethritis in men at the Genito-Urinary Medicine Clinic Kuala Lumpur Hospital. Med J Malaysia. 2003
Mar;58(1):21-6.
[15] Schaeffer AJ, Knauss JS, Landis JR, Propert KJ, Alexander RB, Litwin MS, Nickel JC, O’Leary MP, Nadler RB, Pontari MA, Shoskes DA, Zeitlin SI, Fowler JE Jr, Mazurick CA, Kusek JW, Nyberg LM; Chronic Prostatitis Collaborative Research Network Study Group: Leukocyte and bacterial counts do not correlate with severity of symptoms in men with chronic prostatitis: the National Institutes of Health Chronic Prostatitis Cohort Study. J Urol. 2002
Sep; 168(3): 1048-53.
[16] Hennenfent BR, Lazarte A, Feliciano JR AN: Five Men, Mean Age 70, in Acute Urinary Retention, Treated With Repetitive Prostatic Massage and Antimicrobials Combined with Medical Therapy. Publication pending.
[17] Hennenfent BR, Feliciano AE: Changes in white blood cell counts in men undergoing thrice-weekly prostatic massage, microbial diagnosis and antimicrobial therapy for genitourinary complaints. British Journal of Urology. 1998 Mar;81(3):370-6.
[18] Schaeffer AJ, Knauss JS, Landis JR, Propert KJ, Alexander RB, Litwin MS, Nickel JC, O’Leary MP, Nadler RB, Pontari MA, Shoskes DA, Zeitlin SI, Fowler JE Jr, Mazurick CA, Kusek JW, Nyberg LM; Chronic Prostatitis Collaborative Research Network Study Group: Leukocyte and bacterial counts do not correlate with severity of symptoms in men with chronic prostatitis: the National Institutes of Health Chronic Prostatitis Cohort Study. J Urol. 2002
Sep; 168(3): 1048-53.
[19] Hennenfent BR and Hickman CJ: Patient-perceived Efficacy of Prostatic Massage as a Treatment Modality for Prostatitis, Prostatodynia, and BPH: An Exploratory Study. Infections in Urology 2000;13(6):148-164.
[20] Mehik, A., Hellstrom, P., Nickel, J. C., Kilponen, A., Leskinen, M., Sarpola, A. et al: The chronic prostatitis-chronic pelvic pain syndrome can be characterized by prostatic tissue pressure measurements. J Urol, 167: 137, 2002
[21] Schaeffer AJ. Epidemiology and demographics of prostatitis. Andrologia. 2003 Oct;
35(5): 252-7.
[22] Wright ET, Chmiel JS, Grayhack JT, Schaeffer AJ. Prostatic fluid inflammation in prostatitis. J Urol. 1994 Dec; 152(6 Pt 2): 2300-3.
[23] Schaeffer AJ, Knauss JS, Landis JR, Propert KJ, Alexander RB, Litwin MS, Nickel JC, O’Leary MP, Nadler RB, Pontari MA, Shoskes DA, Zeitlin SI, Fowler JE Jr, Mazurick CA, Kusek JW, Nyberg LM; Chronic Prostatitis Collaborative Research Network Study Group. Leukocyte and bacterial counts do not correlate with severity of symptoms in men with chronic prostatitis: the National Institutes of Health Chronic Prostatitis Cohort Study. J Urol. 2002
Sep;168(3):1048-53.